Because the stakes are incredibly high, the mechanisms ensuring that every tablet, vial, and injection meets rigorous standards must be infallible. This mechanism is Quality Control. broader quality management concepts, QC is the “boots on the ground” aspect of quality—the laboratory-based analytical work that acts as the nal gatekeeper before a product reaches a patient.
The distinction between Quality Assurance (QA) and Quality Control (QC) is fundamental to understanding how the industry manages risk in the world of pharma consulting (https://despharmaconsulting.com/guide-to-pharmaceutical-consulting/). While they are symbiotic and often housed under the same corporate umbrella, their functions are distinct. And with the industry growing in many ways (https://www.marketsandmarkets.com/Market-Reports/pharmaceutical-quality-management-software-market-79122728.html), it is more important than ever to master the nuances here.
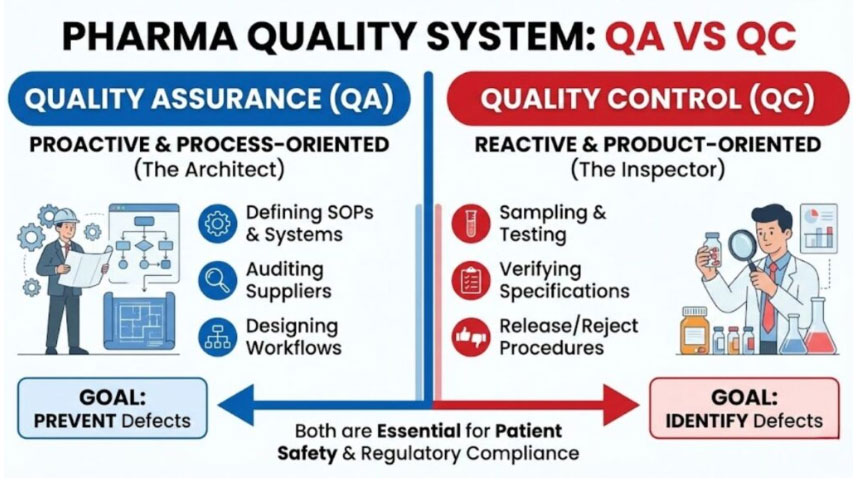
Quality Control (QC), conversely, is reactive. It is focused on identifying defects in the actual products produced. QC is responsible for sampling, specifications, and testing, as well as the organization, documentation, and release procedures which ensure that the necessary and relevant tests are actually carried out. QC is the “inspector” that tests the final build to ensure it matches the blueprints perfectly. A robust pharmaceutical quality system requires both a strong architect (QA) and a rigorous inspector (QC).
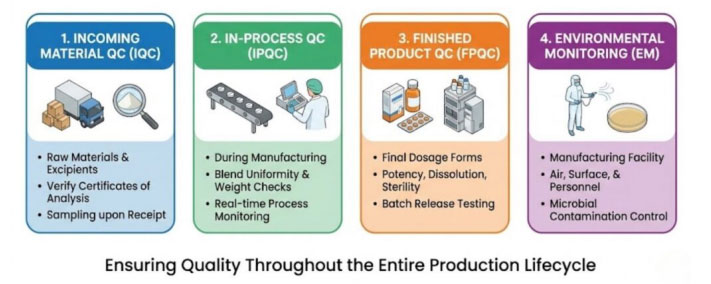
To ensure comprehensive coverage, QC activities are generally categorized into four distinct phases spanning the production cycle. When asking, “What are the 4 types of QC?” in the context of pharma, they typically refer to these critical control points:
Incoming Material Quality Control (IQC): Great drugs cannot be made from poor ingredients. IQC involves sampling and testing Active Pharmaceutical Ingredients (APIs), excipients (fillers, binders), and packaging materials immediately upon receipt. These materials must match their Certificate of Analysis (CoA) and meet internal specifications before being released into the warehouse for use in manufacturing.
In-Process Quality Control (IPQC): Testing shouldn’t wait until the end. IPQC involves checks during the manufacturing process itself. This might include checking the blend uniformity of a powder before it is compressed into a tablet, measuring the pH of a solution during mixing, or verifying the torque of a bottle cap on the assembly line. These checks ensure the process remains in a state of control.
Finished Product Quality Control (FPQC): This is the final battery of tests on the completed, packaged product. It verifies that the batch meets all release specifications for potency, dissolution (how fast it breaks down in the body), sterility (for injectables), and physical appearance. Only after passing FPQC can a batch be certified by a Qualified Person (QP) for market release.
Environmental Monitoring (EM): Especially critical in sterile manufacturing, EM is the ongoing QC of the manufacturing facility itself. It involves testing air particulates, surfaces, and personnel gowning for microbial contamination to ensure the “cleanroom” environment is not compromising the product.
They include:
Cause-and-Effect Diagram (Ishikawa/Fishbone): Used in investigations to identify root causes of a lab error or manufacturing deviation.
Check Sheet: Structured forms for collecting data in real-time on the manufacturing floor.
Control Chart: Vital for monitoring process stability over time, showing if a critical parameter (like tablet weight) is staying within statistical control limits.
Histogram: A bar graph showing frequency distributions, useful for seeing if process data is centered around the target specification.
Pareto Chart: Based on the 80/20 rule, helping QC teams prioritize which types of defects are causing the most issues.
Scatter Diagram: Used to analyze relationships between two variables, such as mixer speed vs. blend uniformity.
Stratification (Flow Chart/Run Chart): Separating data from different sources (e.g., different shifts or machines) to find patterns.
Quality Control does not operate based on internal whim; it is tightly governed by regulatory statutes known as current Good Manufacturing Practices (cGMP). These quality control guidelines are enforced by agencies like the FDA (USA), EMA (Europe), and PMDA (Japan). The FDA’s cGMP regulations specifically delineate the responsibilities of the Quality Control unit. For instance, 21 CFR Part 211 (https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?CFRPart=211) outlines requirements for laboratory controls, testing procedures, and the independence of the quality unit. Failure to adhere to these regulations results in FDA Form 483s, warning letters, or consent decrees.
Furthermore, global harmonization efforts, led by the International Council for Harmonisation (ICH), provide detailed technical guidelines. The ICH Q7 guideline (https://www.fda.gov/regulatory-information/search-fda-guidance-documents/q7-good-manufacturing-practice-guidance-active-pharmaceutical-ingredients-guidance-industry),
The importance of quality control in the pharmaceutical industry cannot be overstated. It is the firewall that protects patients from sub-potent, contaminated, or dangerous medicines. A failure in QC doesn’t just cost money; it damages public trust in science and medicine. Beyond patient safety, robust QC is essential for business continuity. The academic and scientific rigor required for drug development must be matched by equal rigor in commercial manufacturing. Institutions like Purdue University’s Department of Industrial and Physical Pharmacy (https://www.ipph.purdue.edu/) emphasize that understanding the physical and chemical properties of drugs through rigorous analysis is foundational to ensuring consistent manufacturing quality.
Furthermore, the economic implications of poor quality are staggering. Recall costs, litigation, and regulatory shutdowns can bankrupt a company. Research emanating from centers like Johns Hopkins Bloomberg School of Public Health often highlights the critical role of regulatory oversight and rigorous testing standards in preventing adverse drug events that burden healthcare systems.
Ultimately, Quality Control is the translation of the R&D promise into a reproducible commercial reality. As the industry moves toward more complex biologics and personalized medicines, the reliance on highly sophisticated analytical chemistry—a discipline championed by programs at universities like the University of Kansas Department of Pharmaceutical Chemistry—will only grow.
Every pharmaceutical challenge is unique. That’s why we start with a no-obligation consultation to understand your specific needs—whether it’s accelerating timelines, closingcompliance gaps, or optimizing manufacturing operations.